



General Requirements - Clinical Impact
This content includes information linking Environment of Care and Life Safety Code deficiencies and their impact on patient care and patient safety.
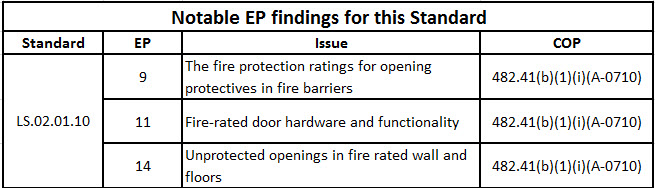
LS.02.01.10: Building and fire protection features are designed and maintained to minimize the effects of fire, smoke, and heat
Clinical Impact
Fire Safety: Background
Fire safety impacts both the lives of the occupants and the physical structures.
Fire Safety: Intent of the Life Safety Code
In our healthcare buildings we strive to protect the occupants by managing fire risk. We also benefit by protecting our financial investments in these healthcare buildings, which allows the organization to continue to achieve its mission and serve patients.
Over the years the healthcare building have benefited from the Joint Commission requirement of complying with the National Fire Protection Association (NFPA) Life Safety Code (NFPA 101-2012) and the associated Life Safety Chapter. Part of the process also includes the proactive use of the Statement of Conditions provided to all Joint Commission accredited organizations.
The specific focus here is on minimizing the effects of fire, smoke and heat. Healthcare buildings are built with a series of fire barriers, designed to restrict the movement of fire in a building. Fire barriers are a system of walls, floors, doors, fire windows, fire dampers, and managed penetrations. The fire barrier is not a single component. If a fire door fails, the fire barrier fails; if there are unprotected openings (i.e. holes) in the fire rated walls, the fire barrier fails.
Most fire-related deaths are not caused by burns, but from smoke inhalation. Property damage is directly related to the fire conditions. Maintaining the integrity of fire barriers first protects the built environment and by default those occupants living in it. [NOTE: In a later module we will explore smoke barriers that are designed to protect occupants lives from smoke inhalation.]
If a fire barrier is more than walls, just what is a fire barrier? As mentioned above a fire barrier is several components, that when properly maintained protect the structure and its occupants. Each component has been tested to establish how much protection can be anticipated.
For example, the fire door is required to have certain features to ensure it will pass testing agency tests, including the door must have either self-closing or automatic-closing devices; functioning hardware, including positive latching devices; and the gaps between the meeting edges of door pairs are no more than ? inch wide with the undercut being < ¾ inch (See LS.02.01.10 EP 5).
In a similar manner the walls that hold the doors must be built to maintain their rating. For the 2-hour fire barrier, the wall construction must also pass the testing agency test. All components that affect the fire barrier must be tested to ensure the fire barrier as a system can perform as required.
If a fire rated door or other fire barrier component were modified, the rating is no longer maintained. For example, if a person applied white surgical tape over the door latch to cause the door to no longer latch, the door would be ineffective in containing fire in a fire condition, allowing the fire to spread. In a similar manner, if a contractor were installing cables above the ceiling and penetrated a rated fire barrier and did not install an acceptable remedy, the entire fire barrier could be compromised.
Suggested Solution to Managing Fire Barriers:
Many organizations use a Barrier Management Program, restricting the access above ceilings to prevent unknown breaches in the fire barriers. This program is discussed in greater detail in June 2012 Perspectives (pages 3 – 5). However, clinical staff can be an important part of the solution as well. Supporting facilities by endorsing the Barrier Management Program is an important first step. But also, supporting facilities by insisting staff do not block fire doors open, do not compromise latching or closing devices and providing support during construction activities.
Building Compartmentation: Defend in Place
Units of Defense: Building Compartmentation
Healthcare occupancies are designed to protect occupants by defending in place, rather than evacuation (as in business occupancy). To accomplish this, healthcare occupancies are designed with certain features that protect the occupants. For this to occur, all features of fire safety, including the building construction and fire suppression/alarm systems, need to be fully operable.
In 1978 the Joint Commission released an LSC model called the Unit Concept. This model was mainly developed to educate the surveyors about the LSC, but when it caught on, the Joint Commission published the concept and used it to teach health care professionals about code compliance. In a health care occupancy, because of the building type and staff-to-patient ratios, the reaction to a fire is to "defend in place."
The Unit Concept includes the following:
- Building unit – The compartmentation of the total structure, including appropriate building construction/type. This is the largest of all units, as it has to do with how well the building will perform in a standard fire. It also includes fire barriers and floor assemblies. Features such as roof construction, fire detection and suppression systems and exiting methods contribute to the building unit.
- Room unit – Individual rooms are the first unit of defense, and the room unit is the smallest of the units in the Unit Concept.The term room unit is somewhat misleading in a non-sprinklered compartment, as there is no requirement for separation between patient rooms. In a sprinklered environment, due to the rapid response of the sprinkler head, the patient room certainly is the first unit of defense. In a non-sprinklered compartment, the original concept of the LSC was to separate use areas (rooms) from the exit access (corridor) to provide an environment free from the products of combustion.;
- Compartment – Based on the size of a smoke compartment (22,500 square feet maximum), this unit component includes rooms and corridors, and creates areas that may be accessed horizontally, which is the preferable method to rapidly move patients. The compartment unit includes all the requirements for separating an institutional occupancy into smoke compartments. The maintenance elements include wall penetrations, smoke dampers, and door hardware. Smoke compartmentalization is one of the most important features in the LSC, and a facility must be diligent in making sure these features are properly maintained.
The smoke barrier is identified as having 30 minute Fire Resistive Rated assemblies, and is easily identified as having cross-corridor doors without latching hardware, but with door closures and a gap at the meeting edges of < 1/8”. The smoke barrier assembly reaches from the outside wall to the other outside wall, from the deck above to the floor, and is to be without unprotected openings. A fire barrier is similar, however a fire barrier must meet certain criteria related to how long the assembly can resist the penetration of fire from one side to another (typically either one hour construction with 45 minute doors; or two hour construction with 90 minute doors). Like the smoke barrier, the fire barrier reaches from the outside wall to the other outside wall, from the deck above to the floor is to be without protected openings. The major difference is that a two hour rated fire barrier can separate building occupancies, provided certain criteria is met. This includes not exiting from a higher occupancy to a lesser occupancy in a fire situation (i.e. not exiting from a hospital occupancy through a business occupancy). However, in certain situations, it is allowable to exit from a business occupancy through a healthcare occupancy. - Floor assembly – Floor assemblies separate floors, with a fire rating determined by the building construction type and height of the building. The floor assembly unit contains the floor slab and all vertical penetrations of that slab. (If the smoke or fire barriers fail, then the floor assembly becomes the next unit of defense. Vertical penetrations of floor assemblies that are improperly maintained can cause smoke and fire to spread vertically throughout the building.) With the necessity to supply many mechanical, electrical, and patient support systems through chutes and shafts, and to provide vertical access by stairs and elevators, a facility must be diligent in making sure vertical penetrations are properly sealed and access panels are appropriately rated. Floor assemblies vertically separate occupancies.
- Exit – A primary feature of life safety is the ability to exit a compartment and, as appropriate, to exit the building. Exits must be maintained so that if a fire (or other incident) occurs, the rapid movement of patients and visitors can take place. In a defend-in-place occupancy such as a health care occupancy, the likelihood of having to totally evacuate a building is rare, but the possibility still exists. Even in a fully sprinklered building, the need to use the means of egress and exits may be necessary due to other internal or external disasters. When an occupant enters this type of component and leaves an unsafe environment, he or she is considered to be out of harm's way. Therefore, exit areas must be considered a priority in a PM Program. The Joint Commission will evaluate business occupancies in regard to the accessibility of the exits. No exit shall be compromised in a business occupancy.