



Protection - LS.02.01.30 - Clinical Impact
This content includes information linking Environment of Care and Life Safety Code deficiencies and their impact on patient care and patient safety.
The organization provides and maintains building features to protect individuals from the hazards of fire and smoke
Principles of Fire Development
For most common fires to burn there must be three elements: ignition source, oxygen and fuel (material to consume). If any one of these are missing, the fire cannot develop. Once ignited, a chain reaction occurs where a fire can be sustained by its own heat and further release of energy and consumption of fuel-oxygen. Fire can be extinguished if any of these are removed. (NOTE: there are certain exceptions to this rule, certain chemicals can generate heat/fire without oxygen, etc.)
Fire Safety: Background
Most fire deaths are not caused by burns, but by smoke inhalation. As the person inhales smoke their ability for self-rescue is diminished to the point where they cannot escape to an exit. As a fire grows it consumes oxygen. When oxygen levels are at 21%, there is normal air to breath; if the oxygen level is reduced to 17% judgment is impaired; at 12% headache, dizziness and fatigue occur; at 9% unconsciousness and at 8% respiratory arrest.
Often the smoke of a fire incapacitates people so quickly that they are overcome and cannot make it to an area of refuge or exit. In the smoke are synthetic materials used in construction and are common in the healthcare environment. These materials are often small enough to affect the respiratory systems protective filters and lodge in the lungs. Some particles in the smoke are also toxic. Mixed with heat, smoke can also create vapors of fog-like droplets of liquid that can poison on contact or if ingested. Finally, toxic gases (i.e. carbon monoxide or CO) can be deadly.
In addition to producing smoke, fire generates heat, which is also a respiratory hazard. Superheated gases burn the respiratory tract. When the air is hot enough, one breath can kill.
Fire Safety: Intent of the Life Safety Chapter, LS.02.01.30
LS.02.01.30 states: the organization provides and maintains building features to protect individuals from the hazards of fire and smoke.
While LS.02.01.10 focuses on the building to protect occupants from fire, Standard LS.02.01.30 focuses mostly on the hazards of fire and smoke. Fire destroys buildings; Smoke kills the occupants. Although fire barriers have higher fire ratings, managing the development of smoke in a fire is also extremely important in saving lives.
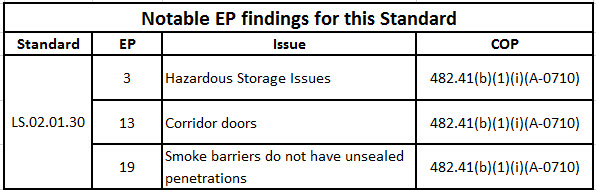
The specific focus is on minimizing the effects of smoke and heat. Healthcare buildings are built with a series of smoke barriers, designed to restrict the movement of smoke in a building. Smoke barriers are a system of walls, floors, doors, smoke dampers, and managed penetrations. The smoke barrier is not a single component. If a smoke door fails, the smoke barrier fails; if there are unprotected openings (i.e. holes) in the smoke barrier walls, the smoke barrier fails.
Most fire-related deaths are not caused by burns, but from smoke inhalation. As a fire develops smoke is generated. Restricting the movement of smoke directly saves lives. Any breach in the smoke barrier system may result in loss of life. [NOTE: In an earlier module we explored fire barriers that are designed to protect occupants lives from fire.]
If a smoke barrier is more than walls, just what is a smoke barrier? As mentioned above a smoke barrier is several components, that when properly maintained protect the structure and its occupants. Each component has been tested to establish how much protection can be anticipated. For example, what does it mean if a smoke door is required? The smoke door must be substantial so LS.02.01.30 EP 20 requires the smoke door be 1-3/4 inches thick with either self-closing or automatic-closing devices and the gaps between the meeting edges of door pairs are no more than ? inch wide with the undercut being < ¾ inch. What is different from a fire door is that the smoke door is not required to latch.
In a similar manner, the walls that hold the doors must be built to resist the passage of smoke. All components that affect the smoke barrier must be able to resist the passage of smoke.